
Recognising typical crisis points during laminitic treatment
By Andrew Poynton FWCF
Poynton Farriery Clinic, Malmesbury, Wiltshire, England.
Farriery is an essential part of recovery of the laminitic along with veterinary care and day to day management of the patient. To qualify the area of discussion a large horse is taken as the example in the scenarios that follow, but the principle is relevant to all laminitics. Ponies that are treated for laminitis are much more resilient due to their lack of weight and although we can help or hinder their recovery, often they will survive irrespective of farriery intervention, whereas horses are far more dependent on positive farriery intervention. Misinterpretation of the cycle of events during the recovery of the laminitic can and does sometimes lead to premature aborting of treatment when crisis points are encountered but not understood.
Laminitis is an emergency, a blue light situation, particularly in the large horse. Why don’t we, farriers and veterinary surgeons, (perhaps we think we do already), agree that we should be trained in effective practices that are likely to improve recovery chances, something proven and positive that we can do? So as soon as laminitis is suspected, we can act positively, without negative side effects, giving the patient a fighting chance from the outset. It seems to me that when the action is initiated way down the road, days, sometimes weeks, so much ground is lost, that time can never be recovered, to the detriment of the horse.
It is important that we understand the effect of the treatment we are administering, as lack of understanding of the application of a treatment or technique can be less than helpful and in some cases dangerous. So we must engage the grey matter before launching into a course of treatment, and then constantly evaluate the results. If there are any negative results arising, stop, investigate, collaborate with the vet, or vet with farrier. The procedure advocated here has been practised and refined for about fifteen years. By applying this in the early stages, freefall destruction can possibly be limited and arrested, as outlined below. We need to be aware of the chain of events that happens in the laminitic, to recognise also that there are varied outcomes likely due to the treatment received. ‘Knowledge is power’, so if we know what is likely to transpire, we can prepare ourselves, we may be able to alter the outcome by pre-empting what appears to be inevitable with positive intervention. We first witness the unstable degeneration and necrosis that occurs within the hoof of the laminitic, but aim to help reverse the trend to regeneration health and stability.
The time-line charts in this article illustrate a variety of scenarios common to the acute laminitic. This isn’t a scientific representation, rather an illustration. I often say to horse owners, ‘your horse is likely to go through a roller-coaster ride on route to recovery’.
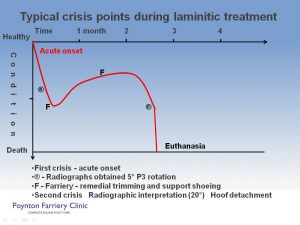
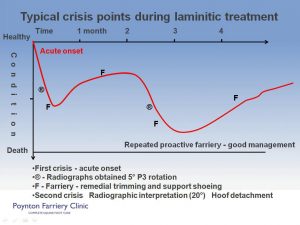
Typical crisis points during laminitic treatment.
This illustration has two different conclusions; the first culminates in euthanasia, based on the deterioration of the clinical condition of the horse and the radiographic interpretation. The conclusion drawn is that the case has deteriorated in all aspects, there is continuing pedal bone rotation, the only humane response is to halt the suffering and destroy the horse. The alternative response at the second crisis point differs in the interpretation of the radiographs by experienced eyes. In this instance the hoof capsule is identified as detaching and migrating away from the pedal bone as expected, phalangeal alignment is fair, so the decision to continue to ‘chase the bone’ (Pedal bone) and treatment as before is made, with a positive outcome.
Obese 17hh show hunter – acute laminitis – 3 scenarios
Scenario 1. Day one, unfortunately this poor horse suffers acute laminitis, he’s obese. He may have equine metabolic syndrome, it might be Cushingoid. The method of farriery intervention is constant irrespective of cause, but what we do to the feet at the different stages of the condition may vary greatly. In this first scenario though there is no farriery intervention. The patient becomes distressed, ischemia at basement membrane level, leading to lamellar breakdown, and we’ll say for argument’s sake, he’s been shod for 8 weeks, due for shoeing, his feet are long and it’s a 17 hand horse. His condition deteriorates; it’s so severe that within 48 hours he’s lying down. The horse is sweating at this stage, and if forced to stand, he’s rooted to the spot. There’s a depression developing at the coronary border from heel to heel. The Vet is eventually called, along with the mobile X-ray unit. Radiographs reveal total detachment of P3 in both front feet. The sole is convex and there is this trench at the coronary border. The horse is in great distress; euthanasia is advised and carried out. End of story, too late. So that’s within days, dead, and the only appropriate treatment in the circumstances.
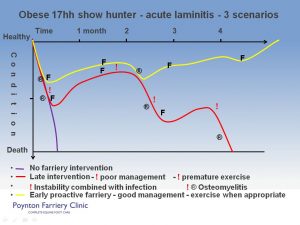
Scenario 2. The same horse, suffers acute laminitis as in the first instance, but after a day, the vet and the farrier are called. The feet are X-rayed; radiographs reveal approx. 5° phalangeal rotation in let’s say the LF and negligible movement in the RF. The hind limbs appear ok so far. The vet administers Bute or whatever pain relief is required, maybe ACP, vasodilators, whatever is appropriate. The farrier takes reference from the radiographs, trims the feet accordingly to attain correct phalangeal alignment, and then moulds on shoes that cradle the frog and will support the weight of the horse, elevating the sole along with shortened breakover at the toe, all with the minimum of trauma to the horse.. The hind feet are trimmed and left without shoes as there is good frog contact and the sole has concavity. The horse is immediately more comfortable, pain level reduces, and he can voluntarily get up, lie down and turn around, but is still a very sick horse. Stable conditions are less than ideal – ‘deep litter’ (muck heap). He steadily improves in mobility; so much so that after a few weeks the owner decides it’s a shame to keep him cooped up and turns him out in the dirt rutted paddock/ cattle yard each day to let him stretch his legs. The horse is treated one more time at 6 weeks. After 5 weeks or so, the horse’s condition deteriorates again. The feet are X-rayed again and 20 degrees of rotation of P3 is measured, the sole bulging and a depression at the coronary border. It’s all becoming quite negative. The feet are trimmed again and shoes fitted to realign the pedal bone with the phalanges. This is an unstable situation. The hoof is sloughing. But the horse is immediately more comfortable. He might go on for a couple of weeks, looking much better. The foot looks ugly on the outside, but he is comfortable, and then, after a couple of weeks, the horse’s condition deteriorates yet again. The sole perforates forward of the frog, this is complicated by deep infection under-running the sole into the pedal bone. Anti-biotics are administered. The horse is in distress and, irrespective of the anti-biotics, the infection cannot be controlled. This scenario is also terminal. The first crisis was the acute onset, second crisis the instability, then the third crisis when the infection could not be brought under control.
Scenario 3. The same horse again, but the management is different this time. The owner notices that the horse has quickly become uncomfortable, unwilling to move, shifting weight. The vet and farrier are contacted that day. The vet x- rays the horse’s feet. The radiographs show that there is already some laminal detachment. The horse’s condition is visibly deteriorating, sweating and looking like a possible colic case. Sedative and other analgesic pain relief are administered. The farrier applies the shoes, as mentioned earlier, with the minimum of fuss, support the frog, elevate the sole, shortened the break-over. No exercise. The stable is clean. . The horse’s diet is reviewed and drastically curtailed. He quickly responds to the treatment, but is still a sick horse. He remains in the stable. In five weeks the Farrier and vet see him again. The feet are re-x-rayed. There is some hoof wall separation. The feet are trimmed to compensate for this. The regime does not change. The horse’s demeanour continues to improve; he is reshod again at another five weeks, ten weeks in and the horse is doing well. Then between shoeings, he’s becomes uncomfortable again; the feet are tested and searched for possible infection and in one foot a pocket of pus is released from the toe . It’s drained at the toe, a localised poultice is applied, within a couple of days he is back looking comfortable again. By this time at the coronary border, an even collar of horn is seen, growing evenly from heel to heel, below which is a fault line, the lower hoof wall is growing at a different angle. The lower hoof wall deviation creates a crescent shape void at the toe until the new aligned horn grows down to the ground. This continues as the horse recovers until following a few months in the stable he is taken out for walks, and then allowed to go loose in a sand arena. Within 12 months the horse has a pair of front feet that appear normal healthy hooves. That horse was not allowed to go anywhere until there was stability and integrity and much more like normal hoof conformation returning. That horse can go back to work as before the laminitis.
Does any of this sound familiar? I’m sure that some of our greatest challenges can become our greatest victories. I can think of one or two Everest’s that to me, as I approached them, appeared very daunting but once I’d figured a way through, I understood more and could face that same challenge again with more confidence.
From an article which first appeared in Forge magazine, August 2013. © Andrew Poynton FWCF
For advice or referral contact…
Imprint Equine Foot Care – Tel: +44 1666 822953
Poynton Farriery Clinic – Website: here